





Infant with febrile neutropenia and a hepatic mass
A 7-month-old girl presents to her pediatrician’s office with a 1-week history of fevers and upper respiratory symptoms. What's the diagnosis?


Figure 1
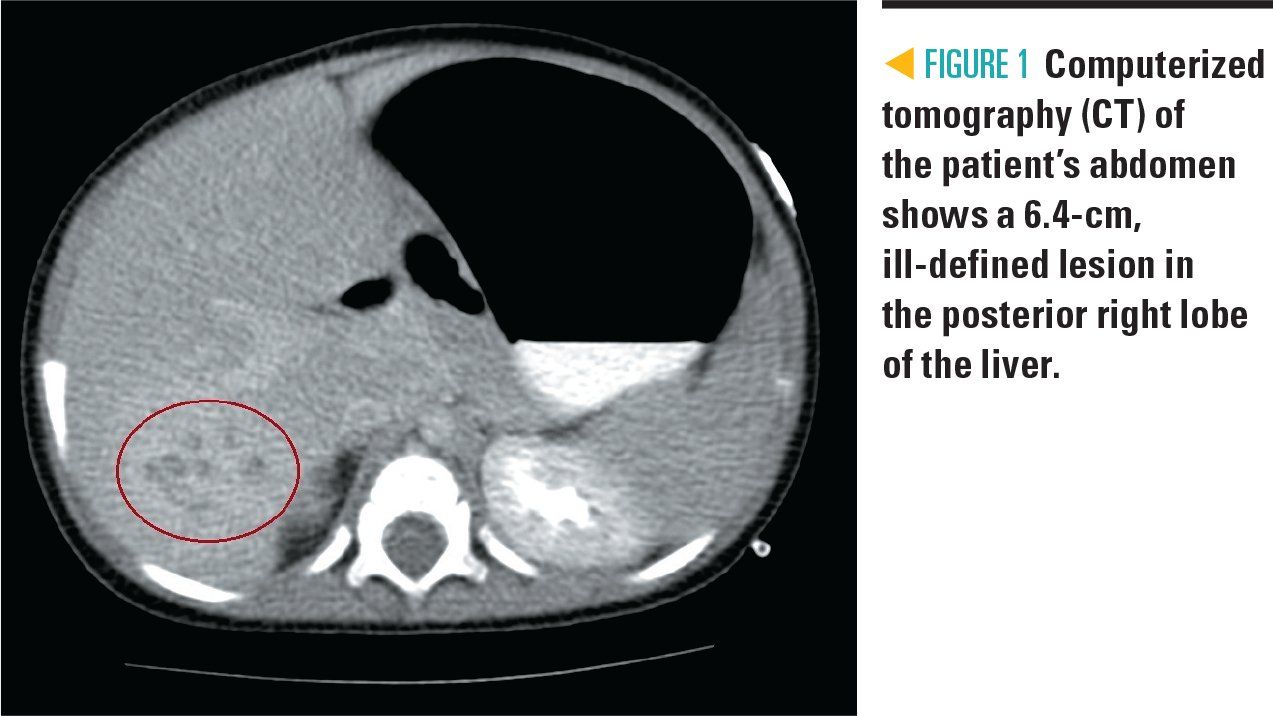


Table 1
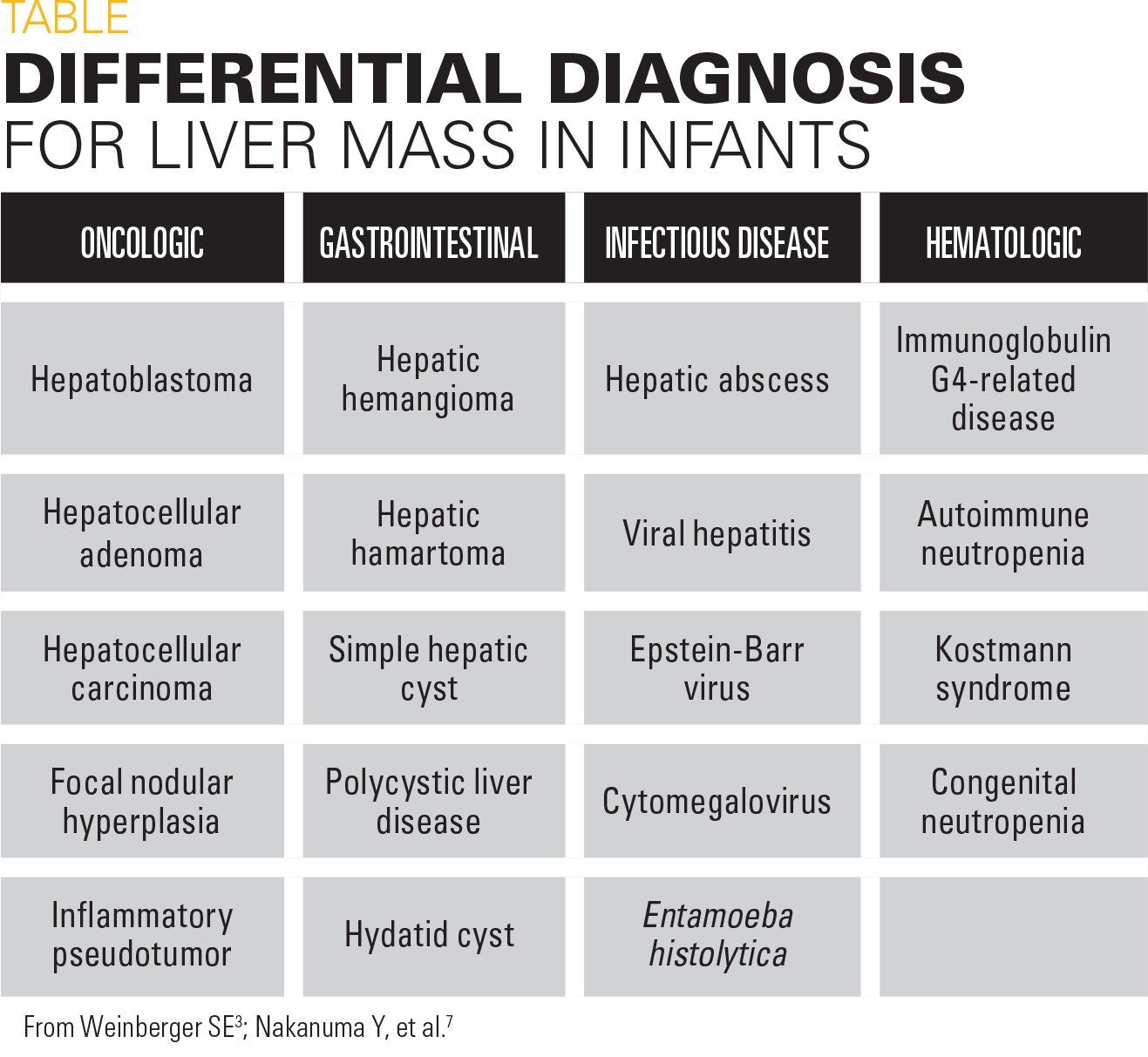


Figure 2
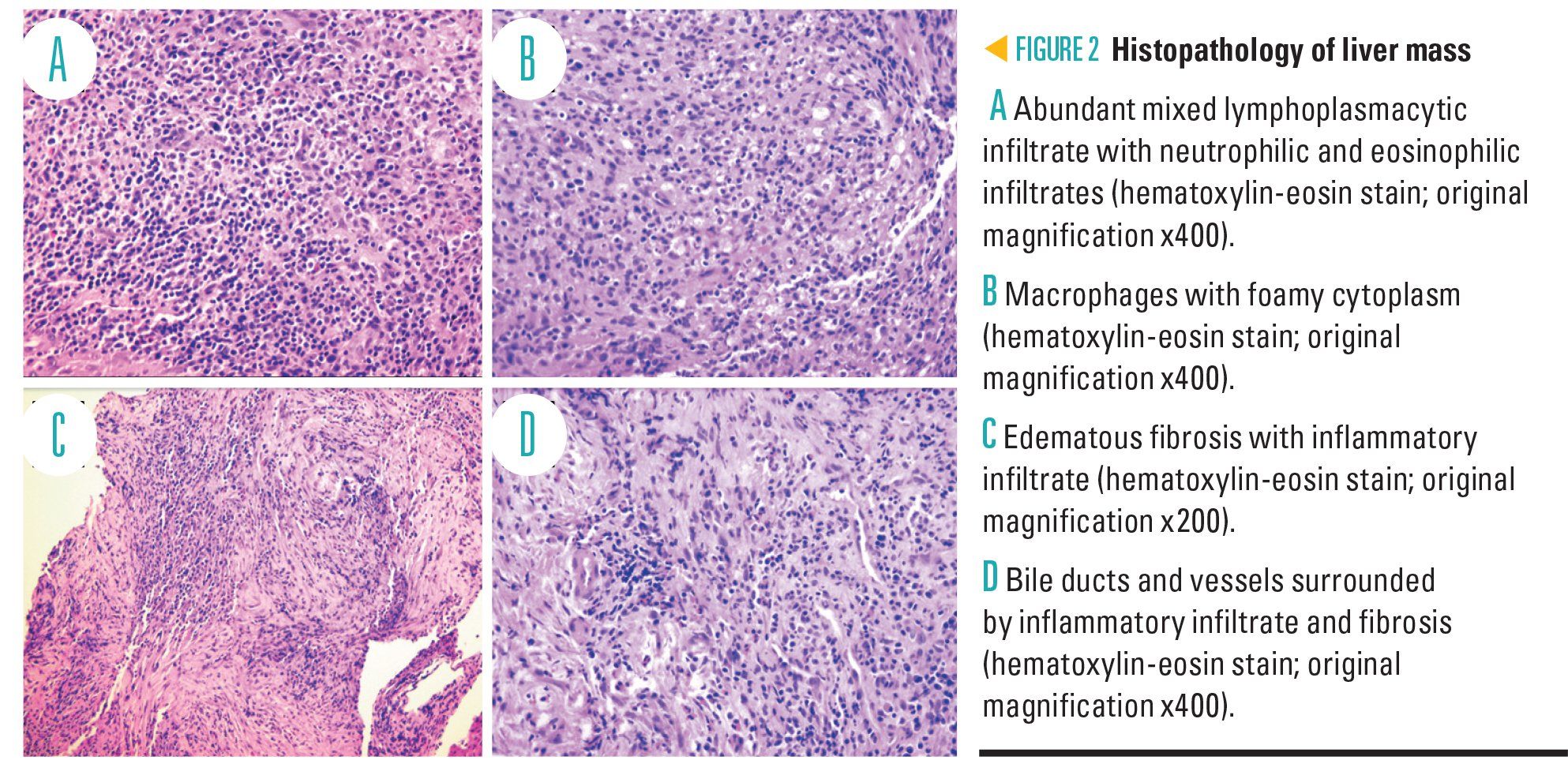


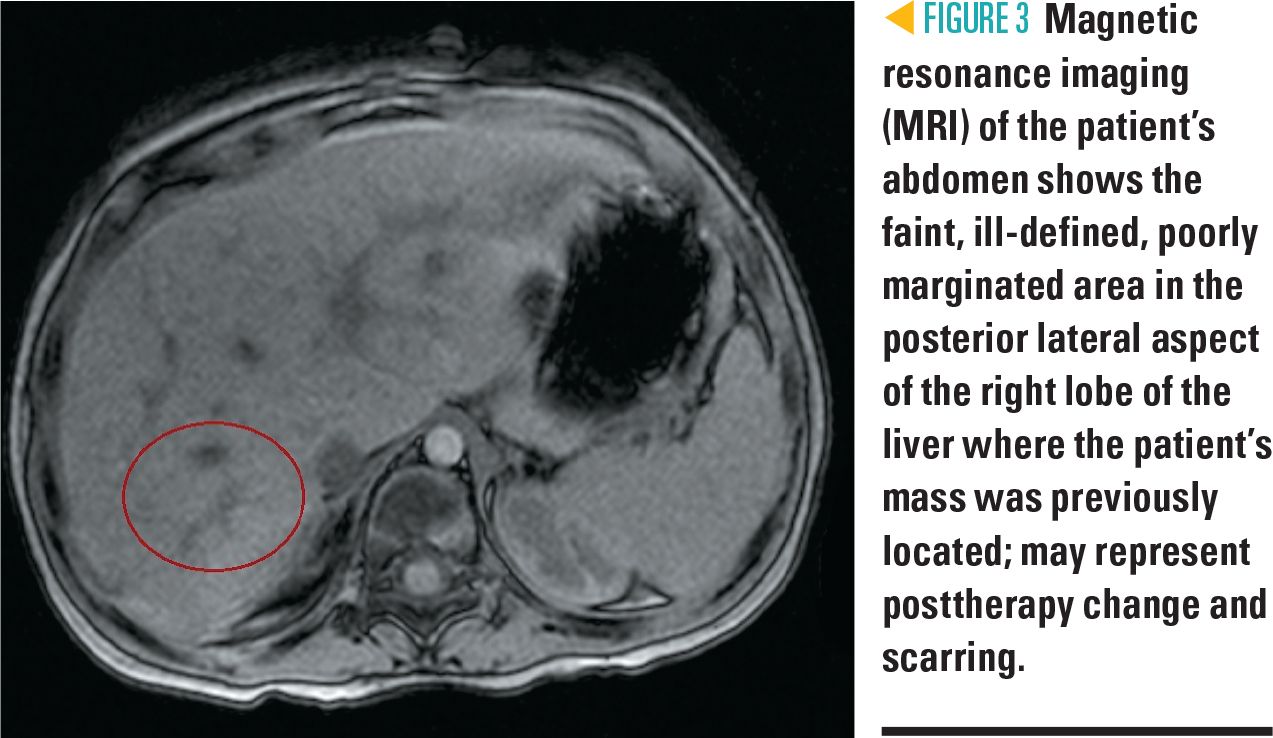
Figure 3
The case
A 7-month-old girl presents to her pediatrician’s office with a 1-week history of fevers and upper respiratory symptoms.
History
The infant had no past medical history and her immunizations were up-to-date. She had some decreased appetite and occasional fussiness, but was otherwise acting appropriately for her age. She had normal urine output. Because of the 1-week history of fevers and rhinorrhea, the pediatrician obtained laboratory studies revealing normocytic anemia and thrombocytosis. The infant was then referred to the emergency department (ED) for further evaluation.
Physical exam
On initial presentation, the patient was febrile to 102.56°F; heart rate was 185 beats per minute; respiratory rate of 36 breaths per minute; blood pressure of 97/49 mm Hg; and oxygen saturation of 99% on room air. Physical exam revealed an active 7-month-old girl in no acute distress but found to be pale and nonjaundiced. She had a regular cardiac rate and rhythm without a murmur. Lungs were clear to auscultation bilaterally without increased work of breathing, wheezing, or crackles. Abdomen was soft, nontender, nondistended with active bowel sounds, and with no hepatosplenomegaly or palpable masses. Her remaining physical exam was normal and appropriate for age.
Labs and hospital course
Initial laboratory results demonstrated a white blood cell count (WBC) of 9.1 K/mcL; absolute neutrophil count (ANC) of 0.3 K/mcL; hemoglobin of 7.8 gm/dL with mean corpuscular volume (MCV) of 79.9 fL; hematocrit, 24.3%; and platelets, 633 K/mcL. Comprehensive metabolic panel was normal, specifically aspartate aminotransferase (AST), 23 unit/L; alanine aminotransferase (ALT), 17 unit/L; alkaline phosphatase, 142 unit/L; and total bilirubin, 0.2 mg/dL.
Inflammatory markers were elevated with C-reactive protein (CRP) of 26.8 mg/dL and erythrocyte sedimentation rate (ESR) greater than 120 mm/h. Iron studies were: iron, 9 mcg/dL; total iron binding capacity (TIBC), 114 mcg/dL; iron saturation, 8%; and ferritin, 434 ng/mL, not exclusively consistent with iron-deficiency anemia. A blood culture and nasopharyngeal respiratory pathogen panel was obtained.
The patient was admitted to the general pediatric unit for febrile neutropenia and was started on cefepime for empiric bacterial antibiotic coverage. Due to potential malignancy, the patient had an abdominal ultrasound that showed a 6.4-cm hepatic mass, confirmed with an abdominal computed tomography (CT) scan (Figure 1).
Differential diagnosis
The patient’s main abnormal vital sign/physical exam finding was fever. She had several initial laboratory abnormalities including severe neutropenia, normocytic anemia, thrombocytosis, and elevated inflammatory markers. Also, she was found to have a nonspecific hepatic mass on imaging, although nonpalpable on physical exam.
This patient’s presentation was concerning for sepsis and malignancy, and thorough evaluation was needed. Such patients require consultation with pediatric subspecialists at the time of presentation, which may require transferring the patient to a tertiary care center. This infant was admitted to a tertiary children’s hospital where subspecialty consultation was readily available. In a patient with fever and neutropenia, prompt initiation of antibiotic therapy for potential sepsis is important, and this empiric coverage should continue until an infectious bacterial process has been ruled out.
For any child who presents with a liver mass, benign or malignant tumors are highly suspected, with malignant tumors being most concerning and requiring prompt evaluation. Hemangioma and hamartoma are the most common liver masses in infants aged younger than 1 year. These lesions often are visualized on abdominal ultrasound, CT, or magnetic resonance imaging (MRI). Hepatoblastoma and hepatocellular carcinoma also are on the differential, which requires a confirmatory biopsy when the patient is clinically stable. Additional imaging may be warranted if there is concern for metastatic disease.
Given the patient's fever, an infectious etiology was suspected, such as abscesses or viral hepatitis, and required further laboratory studies. Although uncommon, Entamoeba histolytica should be considered because of its propensity to form liver abscesses, especially with a history of international travel.
Further evaluation and diagnosis
Febrile neutropenia can be caused by viral suppression of bone marrow function. However, given the additional abnormal findings in this patient (ie, elevated inflammatory markers and hepatic mass), timely involvement of pediatric subspecialists and further workup were needed. The Hematology/Oncology team was consulted for febrile neutropenia, anemia, and thrombocytosis with concerns for a possible oncologic etiology, and the Infectious Disease team for possible infectious process as the cause of her signs and symptoms.
The patient continued to be febrile while on cefepime. Her blood culture was negative. She was found to have enterovirus/rhinovirus on her respiratory viral polymerase chain reaction (PCR) panel, likely the source of her fever. Her remaining infectious disease workup was negative, specifically for hepatitis, Epstein-Barr virus (EBV), cytomegalovirus (CMV), and Entamoeba histolytica. Sepsis was ruled out given that her blood culture was negative. The child remained well appearing throughout her hospitalization and had a negative infectious disease workup.
She underwent a bone marrow biopsy that was negative for malignancy. A fine needle biopsy of the hepatic lesion was performed initially, but this was not diagnostic. Subsequently, she had an open liver biopsy, which demonstrated a right-lobe hepatic mass with pathology showing abundant mixed lymphoplasmacytic infiltrate and positive immunoglobulin (Ig) G4 plasma cells, consistent with inflammatory pseudotumor (Figure 2).
Additional laboratory studies including normal alpha-fetoprotein and beta-hCG levels were negative, but showed positive granulocyte antibodies. Genetic congenital neutropenia panel was also negative. All immunoglobulin levels (IgG, IgM, and IgA) were elevated.
Discussion
Inflammatory pseudotumors (IPT) are rare, benign, solitary, well-demarcated lesions caused by proliferation of inflammatory cells.1-3 Other terminology used to describe IPT includes inflammatory myofibroblastic tumor, plasma cell granuloma, fibrous histiocytoma, fibroxanthoma, and xanthogranuloma. This type of benign lesion is most commonly found in the lung, although extrapulmonary sites have been identified, including the head and neck regions, orbit, major salivary glands, submandibular glands, lymph nodes, breast, kidney, pancreas, gastrointestinal (GI) tract, liver, spleen, retroperitoneum, genitourinary tract, and soft tissue. As of 2011, fewer than 300 cases of hepatic inflammatory pseudotumor have been identified and reported.1 From 1971 to 2008, only 35 pediatric cases were reported with an additional 9 pediatric cases from 2009-2014. Increased IPT identification can be attributed to advances in medical imaging.
Because of a variety of constitutional symptoms (fever, malaise, weight loss, and fatigue) and difficulty in accurately diagnosing IPT, patients often are misdiagnosed initially with malignancy. The majority of documented IPTs are asymptomatic, incidental findings. Although extremely rare, severe lesions causing mass effect have been reported as well.
Initial laboratory studies usually are significant for elevated WBC count, elevated acute phase reactants such as ESR and CRP, and abnormal liver function tests (LFTs). Although uncommon, IPT can cause cytopenias affecting WBC, specifically, neutrophils (ANC), hemoglobin, and/or platelets. Ultrasound, CT, MRI, and positron emission tomography (PET) imaging can demonstrate variable clinical images based on location and density of the affected lesion. If diagnosis remains unknown, patients often undergo fine-needle aspiration (FNA) or open biopsy/resection to determine a diagnosis.
Inflammatory pseudotumor typically develops secondary to an aberrant inflammatory response from a cellular insult. Histologically, when inflammatory cells are activated, various cytokines are produced and released. These cytokines activate neutrophils, eosinophils, lymphocytes, plasma cells, histiocytes, multinucleated giant cells, myofibroblasts, and spindle-shaped cells, leading to cellular damage and IPT formation.1
Although the etiology of IPT remains unknown, several possibilities have been proposed, ranging from postinfectious to autoimmune to neoplastic causes. Inflammatory pseudotumors have been identified after postradiation therapy for malignant neoplasms.4 Several IPT lesions show anaplastic lymphoma kinase positivity at the tyrosine kinase locus, supporting a theory that plasma cell granulomas are low-grade mesenchymal neoplasms with a secondary inflammatory component.3,5
Previously reported cases have not demonstrated a correlation between inflammatory pseudotumor and severe neutropenia, leading to this perplexing case. Generally, patients diagnosed with IPT do not require inpatient hospitalization and can be monitored on an outpatient basis. This patient’s diagnosis remained unknown for multiple days and was complicated by continued fevers and severe neutropenia with initial concerns for malignancy, causing her prolonged hospitalization. The persistent neutropenia was likely secondary to a combination of inflammatory pseudotumor of the liver, viral illness with enterovirus/rhinovirus, and autoimmune neutropenia. Although, the etiology and long-term implications of this patient’s IPT and neutropenia remain unknown, the concomitant presentation suggests a potential association between the two.
Inflammatory pseudotumor can be a manifestation of IgG4-related disease, an immune-mediated condition characterized by lymphoplasmacytic infiltration with a predominance of immunoglobulin G4-positive plasma cells, frequent elevation of serum IgG4, and a dramatic response to glucocorticoids, if administered.6,7 Initially, this patient had elevated serum IgG4 levels, which normalized over time, and liver pathology was positive for IgG4 plasma cells. Given these laboratory and pathology findings, the patient’s IPT appears to be consistent with the lymphoplasmacytic subtype. Although glucocorticoids are found to be effective, this patient did not receive steroids because of her improved fever curve and continued hemodynamic stability throughout her hospitalization.
In most instances of postinfectious neutropenia, particularly with viral infections, neutropenia is transient and rarely results in superimposed bacterial infections. Other viral infections known to cause mild to moderate neutropenia also include influenza A and B, respiratory syncytial virus (RSV), and parvovirus.8 Measles, rubella, and varicella more commonly cause leukopenia with mild neutropenia and lymphopenia. Viruses leading to greater immune suppression include EBV, CMV, human herpesvirus-6 (HHV-6), hepatitis, and human immunodeficiency virus (HIV), which can cause more superimposed bacterial infections.
Previous reports have demonstrated improvements in neutropenia in 3 to 8 days. However, the patient in this case remained persistently neutropenic throughout her hospital course.8,9 Prolonged fevers and neutropenia always raise concern for possible sepsis. Luckily, she was diagnosed with enterovirus/rhinovirus without secondary infectious etiologies.
Autoimmune neutropenia (AIN), caused by granulocyte-specific antibodies, is commonly diagnosed between ages 7 to 9 months.10 Patients often are incidentally diagnosed when laboratory studies are obtained for other reasons with an initial ANC ranging from 0.5 to 1.0 K/mcL.11 Diagnosing AIN can be challenging because of difficulties in detecting autoantibodies, and AIN is most commonly diagnosed with the indirect granulocyte immunofluorescence test (indirect-GIFT) or the granulocyte agglutination test (GAT).11,12 This patient underwent testing and was found to have positive granulocyte antibodies with chronic neutropenia, thereby diagnosing her with a component of autoimmune neutropenia. Treatment typically includes close monitoring with spontaneous remission and disappearance of autoantibodies.10
Patients with recurrent or severe infections or those undergoing surgical procedures often receive filgrastim-G-CSF.12 Escalating therapy for refractory cases include intravenous immunoglobulin (IVIG), corticosteroids, or monoclonal antibodies.10 Although the patient in this case did not have a severe viral infection, she remained persistently neutropenic without improvement, leading to the decision to start treatment with G-CSF.
Among the few reported cases of IPT, even fewer have been associated with neutropenia.13 Cojean and colleagues describe a patient with severe congenital neutropenia concurrently diagnosed with IPT through positron emission tomography (PET) imaging, which occurred after an unsuccessful response to G-CSF in anticipation of bone marrow transplantation (BMT).13 As IPT has not been consistently associated with neutropenia, a plausible connection could be neutropenic patients becoming more susceptible to developing IPT after recovery from a cellular insult secondary to an infection. Although rare, it is important to consider inflammatory pseudotumor when there are concerns for a mass with or without significant neutropenia, as this lesion does not always require inpatient hospitalization, medications, or surgical intervention.
Treatment options
Treatment options are usually conservative but can require surgical resection if no clinical improvement is observed. First-line treatment includes outpatient monitoring with serial imaging, frequent ultrasounds, and repeat laboratory studies. If IPT continues to persist, patients often undergo full resection. After surgical intervention, most cases of IPT do not recur. Nonsteroidal anti-inflammatory drugs (NSAIDs) and antibiotics also have been utilized with varying responses. If an IgG4-related disease is suspected, glucocorticoids can help with tumor regression.4
Patient outcome
During her 19-day hospitalization, the patient’s neutropenia continued and the decision was made to start G-CSF. She was discharged once she was no longer febrile with improvement in her ANC, anemia, thrombocytosis, and inflammatory markers. Because of the location and size of her hepatic lesion, she was not a candidate for a complete resection at the time of her open biopsy. She continued conservative treatment with serial imaging and repeat laboratory studies.
Initially, she was receiving serial abdominal ultrasounds monthly, then extended to bimonthly with an abdominal MRI scan demonstrating complete regression of the hepatic inflammatory pseudotumor 9 months after the initial diagnosis (Figure 2). Luckily, this patient had spontaneous regression and did not require surgical resection of her IPT. She remained on G-CSF for 4 months as outpatient therapy with improvement in chronic neutropenia. Repeat Ig levels also normalized. Overall, her clinical course improved significantly with regression of her IPT and normalization of abnormal laboratory studies.
Acknowledgements: The authors wish to thank Michael Pins, MD, and Christine Salibay, DO, for their contribution to this case report.
References:
1. Al-Hussaini H, Azouz H, Abu-Zaid A. Hepatic inflammatory pseudotumor presenting in an 8-year-old boy: a case report and review of literature. World J Gastroenterol. 2015;21(28):8730-8738.
2. Nagarajan S, Jayabose S, McBride W, et al. Inflammatory myofibroblastic tumor of the liver in children. J Pediatr Gastroenterol Nutr. 2013;57(3):277-280.
3. Weinberger SE. Inflammatory myofibroblastic tumor (plasma cell granuloma) of the lung. UpToDate.com. Avalilable at: https://www.uptodate.com/contents/inflammatory-myofibroblastic-tumor-plasma-cell-granuloma-of-the-lung?source=search_result&search=inflammatory%20pseudotumor&selectedTitle=1~2.Updated May 29, 2018. Accessed June 7, 2018.
4. Adamski JK, Kelsey A, Brennan B. Inflammatory myofibroblastic tumors following the treatment of malignancy in childhood: case reports. J Pediatr Hematol Oncol. 2014;36(2):159-162.
5. Gal AA, Koss MN, McCarthy WF, Hochholzer L. Prognostic factors in pulmonary fibrohistiocytic lesions. Cancer. 1994;73(7):1817-1824.
6. Hirabayashi K, Zamboni G. IgG4-related disease. Pathologica. 2012;104(2):43-55.
7. Nakanuma Y, Ishizu Y, Zen Y, Harada K, Umemura T. Histopathology of IgG4-related autoimmune hepatitis and IgG4-related hepatopathy in IgG4-related disease. Semin Liver Dis. 2016;36(3):229-241.
8. Coates TD. Infectious causes of neutropenia. UpToDate.com. Available at: https://www.uptodate.com/contents/infectious-causes-of-neutropenia?source=search_result&search=viral%20induced%20neutropenia&selectedTitle=1~150. Updated August 16, 2016. Accessed June 7, 2018.
9. Segel GB, Halterman JS. Neutropenia in pediatric practice. Pediatr Rev. 2008;29(1):12-23.
10. Bux J, Behrens G, Jaeger G, Welte K. Diagnosis and clinical course of autoimmune neutropenia in infancy: analysis of 240 cases. Blood. 1998;91(1):181-186.
11. Farruggia P, Dufour C. Diagnosis and management of primary autoimmune neutropenia in children: insights for clinicians. Ther Adv Hematol. 2015;6(1):15-24.
12. Teachey DT, Lambert MP. Diagnosis and management of autoimmune cytopenias in childhood. Pediatr Clin North Am. 2013;60(6):1489-1511.
13. Cojean N, Blondet C, Marcellin L, et al. Successful stem cell transplantation in an infant with severe congenital neutropenia complicated by pretransplant inflammatory pseudotumor of the liver. Bone Marrow Transplant. 2006;38(9):641-643.










11-year-old boy with testicular pain and rash
January 19th 2024An 11-year-old boy presented to the emergency department complaining of left testicular pain for 2 days, described as intermittent and stabbing, which ranged between 5 and 8 of 10 in intensity. Read the full case to see if you can correctly diagnose the patient.

Newborn with midline neck lesion
December 21st 2023A 4-day-old boy with a midline neck lesion was born at term by normal vaginal delivery. After birth, mid line lesion had the configuration of a linear cleft with a cephalocaudal orientation, extending from the level below the hyoid bone to the suprasternal notch with a length of 2.5 cm and a width of 0.5 cm. What's the diagnosis?

A 13-year-old girl with well-demarcated rash on back and chest
October 19th 2023A healthy 13-year-old girl presented with a 1-month history of an asymptomatic, well-demarcated rash on her back and upper chest. The eruption consisted of discrete, dark brown papules that coalesced into large, flat-topped plaques with mild superficial scale and accentuation of skin markings. What's the diagnosis?

Suspicious facial swelling in a 22-month-old girl
October 11th 2023A 22-month-old female patient with sickle cell disease on folic acid and penicillin prophylaxis with a 3-day history of nasal congestion, rhinorrhea, fever and decreased oral intake presents to the emergency department (ED) for acute facial swelling noted when she woke up from a nap. What's the diagnosis?

Friction-induced blistering on a child’s feet
July 14th 2023You are called to the hospital nursery to evaluate a healthy full-term newborn boy who developed painful flaccid blisters and erosions on the tops of his feet and ankles shortly after birth. His mother had a history of similar recurrent skin lesions that healed with scarring. She also had oral and gastrointestinal tract involvement. What's the diagnosis?

