





CPP Patient Case: When to Stop Treatment
Karen O. Klein, MD, and Kent L. Reifschneider, MD, discuss a central precocious puberty (CPP) patient case regarding factors that would lead a physician to either stop treating a patient or continue with treatment.


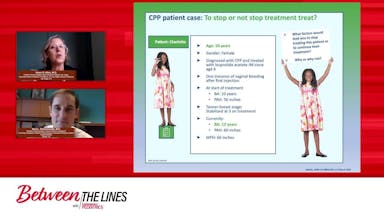
Karen O. Klein, MD: So Charlotte is now 10 years old. She was diagnosed with central precocious puberty and treated with leuprolide acetate since she was 6. So she’s 4 years into treatment. She did have 1 incidence of vaginal bleeding after her first injection. When she started treatment at 6 years old, her bones were 10, so very advanced. This is not a borderline case. This is someone with rapidly progressing precocious puberty. Her predicted adult height was 56 inches. She also has a midparental height of 66 inches. She was in the middle of puberty at 6 years old with stage 3 breasts and she stabilized her physical exam. During these 4 years, her breasts are still stage 3; they’re softer, they’re not stimulated. And now her bone age is 12. She’s predicted now to reach 5 feet, so she’s gained 4 inches of predicted adult height during her treatment. And she’s actually asking you, “Is it time to stop my treatment? I’ve been doing this a long time.” So what things would you look at to decide whether to say yes, you’re ready to stop treatment or no, I would recommend we continue?
Kent L. Reifschneider, MD: This is a great case to talk about the back end. It really highlights some of the key features that we often see every day in our clinics. Really, the crux of the clinical questions that are asked for her, she has been treated for 4 years, which is quite some time. But over that 4 years, she has actually done a really good job. She’s responded quite nicely that over the course of 4 chronological years, her bones have only advanced 2 years.
I think that she has done fabulous. She’s certainly achieved the goals of therapy. Our goal is to slow the maturation of the bones that is noted here that over course of 4 years, the bones only matured 2 years. And of course, this correlates with a considerably improved predicted adult height, so really great response to therapy. But the question is that you proposed is when do we stop? And I think there’s a couple things to think about here is 1, the limitations of the predicted adult heights. So once we stop therapy, what tempos is she going to initiate afterwards.
So excellent question with regards to when to stop therapy especially given the fact that she’s been treated for the last 4 years and is probably has some treatment fatigue. In this regard, she has met all the criteria for treatment, a great response clinically and radiographically. However, the thoughts are, and it’s a judgment by the family and the clinician is the predicted adult height has some limitations. Those limitations consider the tempo in which she was entering puberty at the beginning of therapy, 4 years previous, and 2, the tempo in which she’s going to travel after you stop therapy. So I think those things are that you need to consider when you have this conversation with the family about when to stop therapy, would you agree?
Karen O. Klein, MD: Yes. So the highlights of the benefit to continuing treatment is to continue to improve that predicted adult height. She’s come this far, even though she’s tired, we’ve just shown that more treatment will benefit height further.
Kent L. Reifschneider, MD: Absolutely.
Karen O. Klein, MD: And then if some people might ask about the cost-effectiveness of continuing treatment, well, again, we don’t want to make medical decisions just based on cost. Obviously, we spend lots of money to save lives and to improve patient outcomes, and 1 of the benefits I think we’ve just shown is that the difference in growth potential can be many inches. Some people will say how much is 1-inch worth in dollars, but we’ve just shown, again, the importance of individualizing treatment. This child is predicted at 5 feet right now, 60 inches. But if we stop treatment, she probably will not reach that. So we’ll make that point again to the family she’s done so great, you wouldn’t want to go backwards again. And then the parents—the midparental height is 66 inches. And so is it even possible that we could gain 6 more inches by continuing her treatment. Now in general, that sounds like a lot, and probably the family’s going to be happy if we just gain 2 or 3 more. But when we look at the data I just showed you, some of these children with the good genetic potential as long as we keep that process slow, steady growth, they do gain 5 to 10 centimeters, so as many as 4 and a half inches potentially by continuing treatment past a bone age of 12. So that bone age of 12 has sometimes been a stopping point for clinicians around the country and world, but we’ve just shown that at bone age of 12, you can still gain 5 to 10 centimeters in some cases. Now not everyone, so again, we’re looking at each patient and this particular patient is doing extremely well so there’s no reason to suspect she wouldn’t continue that.
Kent L. Reifschneider, MD: And I think that’s exactly your point. She’s had such a great response just like in other conditions that we treat that are relating to growth, those kids are demonstrating a great response. Why would you want to lose the momentum that you have achieved, right? So I absolutely concur with you, Dr. Klein, is that I would really encourage this family that Charlotte has done such a great job responding and all the momentum that we’ve gained, I wouldn’t want to risk losing it, let alone the fact that I think that she’s probably going to be 1 of those individuals that are going to continue to gain a lot of recovery in height.
Karen O. Klein, MD: So before you saw this data, when you looked at a patient and she got to a point that her bone age was 12 or more, did you use that as 1 of your criteria to consider stopping treatment?
Kent L. Reifschneider, MD: I did to some degree because of the publication in 2018 did talk about that to some degree. So that was brought to my attention, having read that journal, but I think with Charlotte’s case, I think she’s such an outlier that I think she’s pretty easy to distinguish that she’s probably going to continue to benefit. I think that there are some out there that it’s a little bit grayer, a little bit harder to tell because the recovery responsiveness to therapy is not so obvious. And in part, I think with Charlotte, she’s been treated for quite some time, and we know that 1 of the best predictors of outcome with predicted height relative to midparental height is the duration of therapy, right? And I think that’s part of this whole conversation is the duration is the tail end too. That’s part of duration, right? And so she, I think, Charlotte, is an easy case, but there are some that’s not so cut and dry that I really kind of hem and haw on when do we do the call it quits because knowing that duration is such a critical point.
Karen O. Klein, MD: Yes. Thank you. So, and now that you’ve seen some data to support the growth continuing after bone age of 12, will that change your sort of general thinking of the bone age of 12 isn’t as hard of a line?
Kent L. Reifschneider, MD: Yes, yes. And I think that this is a question that we’ve always had as pediatric endocrinologists, and again, their publication is helping to answer that question. And I think that people need to be mindful that there is not a hard stop, a hard start, or line in the sand that you start or stop for therapy because it has to be individualized. And I think that us as clinicians who are helping the child and the family in front of us, we need to take them into consideration and not just data, absolutely.
Karen O. Klein, MD: And now we—yeah. And now we have data to support that thought that we’ve been having, and I think it is important. So having, you know, listened to everything and looked carefully at this new paper, do you have any questions for me for our discussion today?
Kent L. Reifschneider, MD: No. I think that your paper has really been long overdue, and I love the fact that you guys try to tackle the 2 really hard questions. When is it too late to start therapy? And when is it the benefits versus the risk to stop therapy? And I think this publication really starts to help bring some clarity to those questions and help us all to remember that there is not a line in the sand on either end, and then that there are some kids who definitely continue to benefit from ongoing therapy, absolutely.
Karen O. Klein, MD: Well, it was so nice talking to you today and going back and forth on our thoughts about these patients and look forward to seeing you in person sometime.
Kent L. Reifschneider, MD: I can’t wait.
Newsletter
Access practical, evidence-based guidance to support better care for our youngest patients. Join our email list for the latest clinical updates.




