





Painful passage of vaginal mass after discontinuing OCP
Can you diagnose the patient in this edition of puzzler?
Case presentation
A 12-year-old female presented to the emergency department (ED) after 2 days of heavy vaginal bleeding and severe lower abdominal pain that resolved with passage of a large mass. Three months earlier, she had presented to the ED with heavy menstrual bleeding and dysmenorrhea. Laboratory tests revealed severe anemia, but her thyroid panel, von Willebrand factor, prothrombin time test/international normalized ratio, and comprehensive metabolic panel results were all unremarkable. After treatment with intravenous estrogen and transfusion of 2 units of blood, she was discharged home with an oral contraceptive pill (OCP) prescription (standard combination estrogen-progesterone pill) and was advised to take iron supplements and follow up with a gynecologist. The follow-up visit was unremarkable, and the gynecologist advised her to continue the OCPs. She was also advised that if she experienced any breakthrough vaginal bleeding, she should stop taking the OCPs for 4 days and then resume.
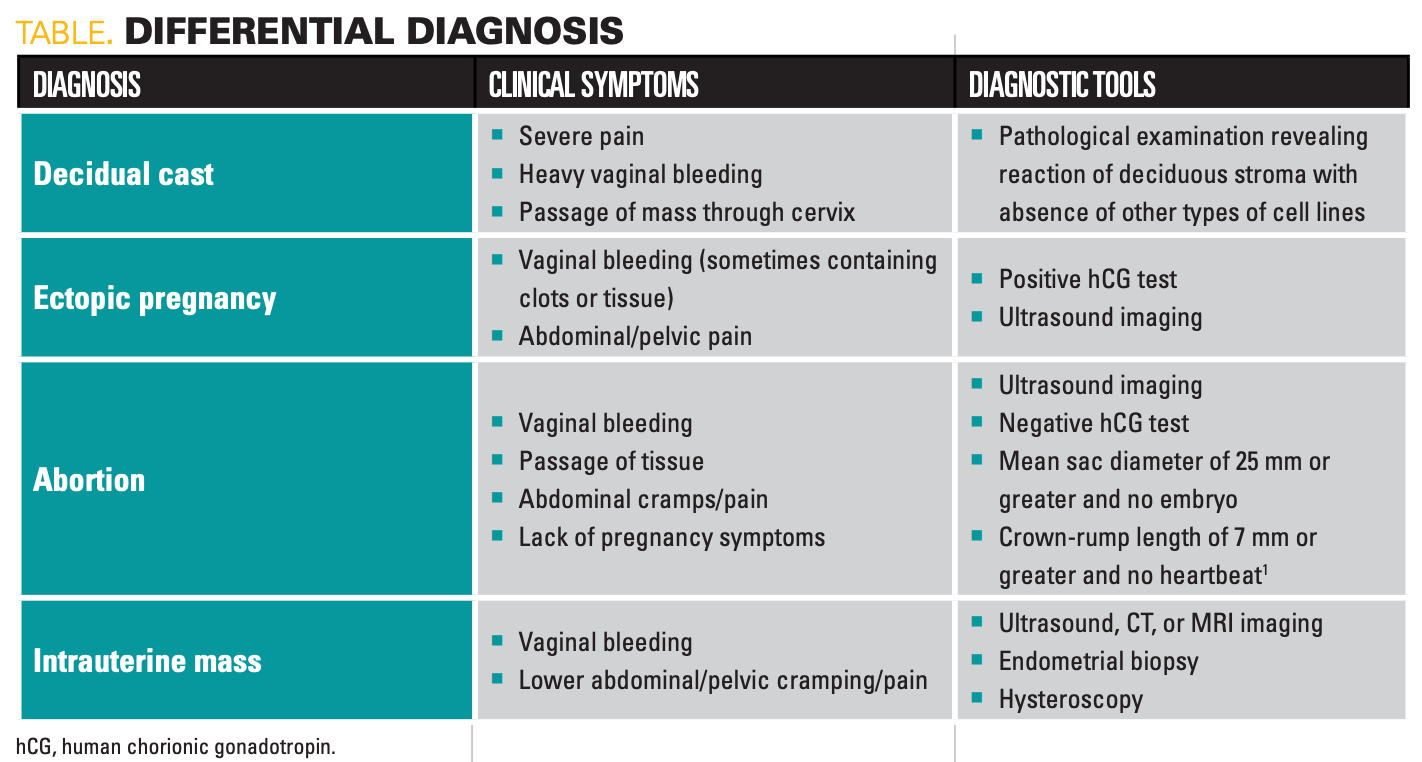
Three days before the current presentation, she began experiencing breakthrough bleeding and stopped taking the OCPs as advised. The next day, she began to have severe lower abdominal pain and cramping in addition to her vaginal bleeding. On day 3 off OCPs, she passed a large mass at the height of the pain (Table). The pain resolved almost immediately after passage of the mass, and she went straight to the ED.


Click image to Zoom
History and examination
Vital signs in the ED were as follows: temperature, afebrile; pulse, 112 bpm; blood pressure, 136/78 mm Hg; respiratory rate, 18 bpm; and oxygen saturation, 100%. She generally appeared uncomfortable but nontoxic. Social history was unremarkable; she reported that she had never been sexually active, and there was no reported history of sexual abuse. Family history was noncontributory. Menarche occurred at 10 years of age. She reported no vaginal discharge aside from the bleeding, and she denied dysuria, frequency, and urgency. Physical examination of her head, eyes, ears, nose, throat, neck, cardiovascular system, pulmonary system, and extremities was normal. Gynecological examination revealed Tanner stage 4 pubic hair, normal pubertal external genitalia, and a small amount of bleeding from the vaginal vault. There was no evidence of trauma on the external exam. No internal exam was performed because she had never had sex. The pediatric emergency medicine (PEM) physician ordered a complete blood count, which came back normal.
Treatment and follow-up
The patient and her mother were told that the mass she had passed was likely a large blood clot. The patient was discharged home with instructions to refrain from restarting the OCPs until she followed up with her obstetrician-gynecologist. The PEM physician declined an offer from the patient’s mother, a family medicine physician, to view the mass or photos of it. The PEM physician did not perform a gynecological examination, did not ask the patient’s mother to leave the room to take a sexual history, and did not order a pregnancy test until prompted by the patient’s mother (this test was negative).
The patient followed up with her pediatric/adolescent gynecologist 4 days later. The patient and her mother were informed that a transabdominal pelvic ultrasound and pathology on the mass should have been ordered. The ultrasound at her follow-up appointment revealed a thick endometrial lining but still within normal range. Pathology report of the tissue mass showed “necrotic luteinized endometrium and inactive glands consistent with oral contraceptive use,” consistent with a decidual cast. The patient was informed that decidual casts are rare and that it was extremely unlikely to recur. She was advised to resume taking the same OCP. At 3-month and 6-month follow-ups, she was doing well and had not experienced any similar episodes of membranous dysmenorrhea.
Discussion and conclusions
Normally, the endometrial lining thickens throughout the uterine cycle and is then broken down and shed during menstruation.1 However, in rare cases, the endometrial lining of the uterus builds up (decidualization) from the effects of progesterone and sheds in 1 piece, forming a cast in the shape of the uterus. These casts are often associated with progesterone therapy (monotherapy is more common but can also occur combined with estrogen), as seen in this patient as well as with ectopic pregnancies, and are the most common cause of membranous dysmenorrhea.2,3 Patients usually experience severe pain as the mass passes through the cervix. After passage of the cast, there are typically no complications, and recurrence is rare. Although decidual casts are benign, the fact that their presentation can closely imitate potential medical emergencies, such as ectopic or aborted pregnancy, makes proper diagnosis essential.4 Decidual casts are extremely rare; one review looking specifically at pediatric populations found only 14 reported cases, mostly associated with OCPs.4
Although the pathophysiology of decidual casts is largely unknown, there are several theories regarding their development, including etiologies related to infection, prostaglandin production, and integrin cell-cell adhesion events.2,5 One of the most common theories suggests that cast formation is related to thickened endometrium caused by an increase in estrogen and/or progesterone levels, potentially linking decidual cast incidence to OCP use (especially given progesterone’s role as the primary decidualizing factor of the endometrium).6 Nearly all reported cases have been linked to use and/or sudden discontinuation of OCPs. Very little information exists regarding decidual cast prevalence or incidence, and reported patients range in age from puberty to late reproductive years.6 Diagnosis is confirmed via pathological examination of passed tissue using a combination of macroscopic features and microscopic identification of a reaction of deciduous stroma with absence of other types of cell lines.5
In this case, the adolescent patient’s complaint was minimized by her health care provider in the ED and a thorough evaluation was delayed, which led to requiring advocacy from her parent and follow-up with her obstetrician-gynecologist. Results of several studies have shown that adolescents, especially female adolescents, are likely to experience dismissal of their pain. A 2018 study published in The Clinical Journal of Pain found that 1 in 10 young adults reported at least 1 instance of dismissed pain, with 30% of these dismissals coming from a physician (parents composed the majority of dismissers) and females reporting being dismissed nearly 3 times as often as males. These instances were also strongly associated with long-term negative psychosocial impacts such as self-directed negativity and feelings of isolation.7 A similar 2017 study published in the Journal of Child Health Care found that female adolescents were more than 2 times more likely to experience pain dismissal, particularly from physicians.8 Given these findings, it is clear that this case of a female adolescent presenting with a decidual cast had the unfortunate combination of factors leading to dismissal of her pain and experience, leaving her with fear and uncertainty about her condition. Strong advocacy from both the patient and her parent was required to receive proper evaluation and diagnosis.
We recommend that health care professionals of all fields improve their awareness of potential biases against groups such as women and adolescents to provide competent, patient-centered care. We also recommend that ED physicians receive better education on the proper evaluation of potential decidual casts, including pregnancy testing, tissue examination, and pelvic imaging.
References:
- Early pregnancy loss. American College of Obstetricians and Gynecologists. 2021. Accessed July 11, 2024. https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2018/11/early-pregnancy-loss
- Malik MF, Adekola H, Porter W, Poulik JM. Passage of decidual cast following poor compliance with oral contraceptive pill. Fetal Pediatr Pathol. 2015;34(2):103-107. doi:10.3109/15513815.2014.970263
- Sen Y, Cimbek EA, Uğraş NS. Decidual cast after discontinuation of oral contraceptives use in a young girl. J Pediatr Adolesc Gynecol. 2013;26(6):e127-e129. doi:10.1016/j.jpag.2013.04.011
- Parkes P, Trainor JL, Raval M, Dhar CP. Endometrial cast expulsion: a rare cause of pelvic pain case report and review of the literature. J Adolesc Health. 2021;68(5):1017-1019. doi:10.1016/j.jadohealth.2020.08.035
- Nunes RD, Pissetti VC. Membranous dysmenorrhea – case report. Obstet Gynecol Cases. 2015. Accessed July 11, 2024. https://clinmedjournals.org/articles/ogcr/ogcr-2-042.pdf
- Brandão P, Portela-Carvalho AS, Oliveira C. Non-painful out of pill membranous dysmenorrhoea. Obstet Gynecol Cases. 2018;rev 5:137. doi:10.23937/2377-9004/1410137
- Defenderfer EK, Bauer K, Igler E, Uihlein JA, Davies WH. The experience of pain dismissal in adolescence. Clin J Pain. 2018;34(2):162-167. doi:10.1097/AJP.0000000000000530
- Igler EC, Defenderfer EK, Lang AC, Bauer K, Uihlein J, Davies WH. Gender differences in the experience of pain dismissal in adolescence. J Child Health Care. 2017;21(4):381-391. doi:10.1177/1367493517727132







Newsletter
Access practical, evidence-based guidance to support better care for our youngest patients. Join our email list for the latest clinical updates.





Having "the talk" with teen patients
June 17th 2022A visit with a pediatric clinician is an ideal time to ensure that a teenager knows the correct information, has the opportunity to make certain contraceptive choices, and instill the knowledge that the pediatric office is a safe place to come for help.




