
The mother of a 4-year old girl complained that the child had been "pulling at her bottom" for several weeks, presumably imitating her younger brother. Visual inspection of the area revealed the real problem.
The mother of a 4-year old girl complained that the child had been "pulling at her bottom" for several weeks, presumably imitating her younger brother. Visual inspection of the area revealed the real problem.
Rarely encountered these days, scarlet fever is believed to be caused by sensitization to an erythrogenic toxin produced by strains of group A beta-hemolytic streptococci.

A right parietal cephalhematoma was first noted on this 2-week-old girl 2 days after her birth.

A 2-day history of fever and sore throat and an erupting rash prompted the mother of a 5-year-old boy to bring her son into the office for evaluation.

This picture shows an unusual linear white object positioned vertically at the center of the posterior pharynx of a 5-year-old girl’s throat.

Erythematous pustules and papules with some coalescence developed on the anterior trunk and to a lesser degree on the face and extremities of a newborn boy the day after birth. The baby was born at full term after an uncomplicated pregnancy and delivery.
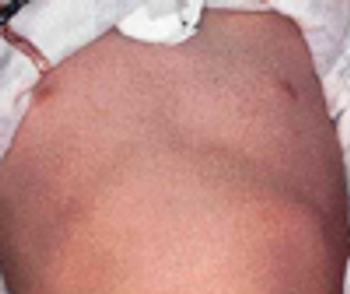
Numerous brown macules were sparsely distributed over the torso, head, and extremities of an African American newborn. The infant also had a mongolian spot on the buttocks. The baby's mother, a great aunt on the father's side, and the great aunt's daughter and grandson had similar brown macules at birth. All family members were healthy.
This fairly common phenomenon, also known as Mongolian spots, affects more than 90% of African Americans, 80% of Asians, 46% of Hispanics, and fewer than 10% of Caucasians.1 The bluish gray or slate-colored areas occur most frequently on the lower back and buttocks and less frequently on the posterior thighs, legs, back, and shoulders. The face is rarely affected. The skin coloration is believed to be caused by melanocyte migration arrest from the neural crest to the epidermis.
The infant's father and sister had similar toe deformities. Radiographs of the feet revealed no bone abnormalities. The patient was referred to a pediatric orthopedist to reassure the mother.
On close inspection, the base of the triangular, seemingly asymptomatic lesion (shown here with the infant lying on her belly) was anterior to the anus on the perineal median raphe. The lesion was excised in the office using local anesthesia, and the opening was sutured with 3.0 chromic catgut. The area was cleaned with warm water until it healed several days later.
This self-limited unilateral dermatitis of unknown cause usually affects preschool children.1-3 Girls are 2 to 3 times more frequently affected than boys.4 The eruption consists of flat-topped pink or flesh-colored papules with a fine scale that form a linear band of less than 1.2 cm in width. It often follows the lines of Blaschko and may extend the entire length of an extremity.
This skin abnormality is cutis marmorata-a physiological dilatation of capillaries and venules of the trunk and extremities in infants and young children caused by exposure to cold. The discoloration fades with warming, as was the case with this baby. The condition is seen especially when subcutaneous fat is decreased.
Photo A shows a red, slightly raised, 1 3 2-cm lesion on the left buttock of a 3-month-old boy. The lesion had been present since birth and had enlarged as the child grew. Photo B shows a similar lesion in the vulva of a 2-month-old girl that also had been present since birth; the mother stated that it had not enlarged.
A 2-week-old infant was assessed for an abnormal penis with a dorsal hood and a meatus that extended to the corona. Both testes were palpable in the scrotum. No chordee was apparent. Hypospadias occurs in 1 in 250 male newborns.1 In neonates with this congenital anomaly, the urethral meatus is ectopically positioned to open proximal to the normal site and on the ventral aspect of the penis or, in severe cases, on the scrotum or perineum. The prepuce is incompletely developed over the glans and presents as a hood. Some cases are associated with a chordee, which causes a ventral curvature of the penis with erection.
This lacy, purplish skin discoloration was noted on the trunk and lower extremities of a 6-week-old boy during a well-baby visit. The mother had noticed the discoloration periodically since birth. It was most apparent when the baby was cold.
A 4-year-old boy presented with a pustular rash on the radial aspect of the right wrist. The rash appeared about 4 days earlier as a group of vesicles on an erythematous base. The lesions caused mild discomfort.
The pearly papules on the cheeks (A), ear, and scalp (B) of 2 newborns are classic presentations of milia. The white or yellow papules range from 1 to 2 mm in diameter. They result from retained keratin and sebaceous material in pilosebaceous skin. The lesions commonly affect the face and may be present at birth or develop within the first few days of life.
Photoclinic: Sucking Blisters
The lesion on this 6-year-old boy occupies almost the entire left side of his nose. The mother attributed it to an injury her son had sustained 2Z\x weeks earlier, when he was hit in the face by a baseball. The sharply defined, slightly elevated, pink macule had fine papules with an annular flat area at its inferior central aspect. A potassium hydroxide preparation of scrapings from the lesion was negative for hyphae. However, fungus culture grew Cladosporium species.
The parents of a 7-year-old girl, who had fallen off her bicycle and hit her left forehead 2 weeks earlier, brought their daughter to the emergency department after she began having increasingly severe headaches. She had been healthy before her fall and had no history of other trauma or meningitis. She had no neurologic deficits on presentation. Examination of the fundus revealed no papilledema.
These pinpoint pustules, some with excoriations, and surrounding erythema appeared on the posterior trunk (A) and outer arms (B) of a 15-year-old boy after he had wrapped his upper body in a wool blanket. These lesions were occasionally pruritic, especially on the arms, where most of the excoriations were noted.
The irides of a legally blind 19-year-old woman had been absent since birth. When she was 6 weeks old, her parents noted that she was not focusing on objects the way her siblings had. They consulted an ophthalmologist who diagnosed aniridia. The woman is able to read book print close up and can ambulate independently, although she has difficulty at times, such as when stepping off a curb in unfamiliar surroundings.

Complaints of pain in an ear prompted the mother of a 4-year-old boy to seek medical consultation for her son. The external ear was red, swollen, and warm. This appearance is typical of erysipelas caused by group A β-hemolytic streptococci.
May 1st 2005
July 1st 2007
February 1st 2007
December 1st 2006
April 1st 2006
May 1st 2006