
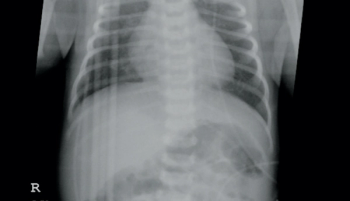
A previously healthy 16-year-old female patient presents with intermittent pleuritic chest pain and shortness of breath. The night before her symptoms started, she hit her chest on a door after a "fainting" episode.
A previously healthy 16-year-old female patient presents with intermittent pleuritic chest pain and shortness of breath. The night before her symptoms started, she hit her chest on a door after a "fainting" episode.

In a newborn nursery, a newborn boy shows signs of irritability, high tone, and tremors on day of life 1. His mother’s past medical history is significant for preeclampsia, previous opiate and cocaine abuse, and current tobacco use and she was incarcerated during the pregnancy. What's the diagnosis?

A 17-year-old boy presents with linear brown spots on his abdomen and chest that developed when he was on a beach vacation with his family the week prior. What's the diagnosis?

A 2-year-old girl with a 36-hour history of left shoulder redness and pain. She developed a fever 24 hours prior to presentation. She was stung by a hornet on multiple areas of her left upper extremity 10 days earlier. What’s the diagnosis?

A 3-week old girl comes to an emergency room with vesicular eruptions and recent mild nasal congestion and fussiness. What’s the diagnosis?

An otherwise healthy 6-month-old boy has a 1-cm area of recurrent blistering with surrounding erythema on his right cheek that developed shortly after birth.
A 6-year-old boy presented to his pediatrician with clear drainage from his left eye for 1 to 2 days. He denied itchiness, pain, vision changes, nasal congestion, or history of allergies. What's the diagnosis?

An adolescent boy developed an asymptomatic brown plaque on the back of his leg. He recently noted the growth of coarse hairs within the lesion.

A newborn boy born via normal vaginal delivery at 38.6 weeks gestation to a 33-year-old G5P2022 mother presented at birth with an asymptomatic 8-mm red, papulonodule with central crusting on the right cheek. What's the diagnosis?

During the evaluation of a healthy 7-year-old boy, an asymptomatic brown “dirt-like” rash is found on the anterior neck. It has progressed over the last 2 months and does not clear with routine bathing and aggressive scrubbing by his mother with soap and water.

The parents of a healthy 20-month-old boy ask for advice about a birthmark on his lower back. The lesion is asymptomatic and has grown proportionately with their son. What's the diagnosis?

A full-term male infant was born at 40.3 weeks gestational age via vaginal delivery to a 29-year-old single G6 P30204 mother with limited prenatal care (3 visits) and short interval pregnancy. The delivery was precipitous: Rupture of membranes was 3 hours in duration with clear fluid; no intrapartum medications were administered; and the infant’s Apgar scores were 9 and 9 at 1 and 5 minutes, respectively. What's the diagnosis?

A healthy 11-year-old boy presents for evaluation of thick skin over the metacarpal (MCP) and proximal interphalangeal (PIP) joints on his right hand. What's the diagnosis?

A 17-month-old African American girl, with no significant past medical history, is brought to the Pediatric Emergency Department with acute onset of swelling in the floor of her mouth. What's the diagnosis?

Anxious parents present their healthy 9-year-old son for evaluation of a slowly enlarging plaque that began developing on his lower back 3 months ago. What's the diagnosis?

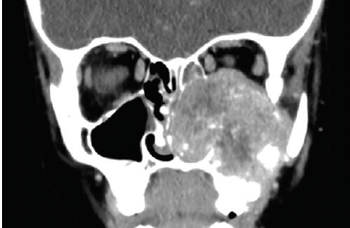
A 9-year-old female presents to the clinic with facial edema that has progressively worsened over a period of a few weeks. What's the diagnosis?

The parents of a healthy 8-year-old girl are worried about an asymptomatic red spot on their daughter’s left cheek that has been enlarging for more than a year. What's the diagnosis?

A 4-year-old boy presents for evaluation with painful swollen fingers on both hands that erupted after he made a snowman with his siblings following a snowstorm. He complains that they are itchy and painful. What's the diagnosis?
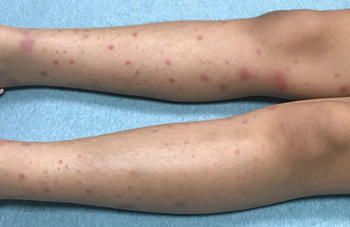
An 8-year-old, previously healthy girl presents to the emergency department (ED) with a rash “that looks likes bruises” and joint pain. The red patchy rash is not painful and not pruritic. What's the diagnosis?

A healthy 6-year-old boy presents for evaluation with a 3-month history of an asymptomatic rash extending from his left thumb to his left wrist. What's the diagnosis?

A 9-year-old girl presents with a painful blistering patch on her right leg noted when her mother picked her up from school following an after-school ski club trip. What's the diagnosis?

A healthy 15-year-old girl presents for evaluation of itchy, painful bumps on her toes that developed 3 weeks earlier. The bumps become more numerous and bothersome when she is outdoors sledding and skiing. What's the diagnosis?

A healthy 10-year-old male presents for evaluation with a 3-year history of an asymptomatic and progressive, mildly pruritic rash over his head and trunk. The first lesion appeared on his back 3 years ago, and numerous other lesions developed insidiously afterward. The patient’s father states that the lesions fade during the winter and become more prominent during the summer. Failed treatment included hydrocortisone. What's the diagnosis?

A mildly overweight 8-year-old Hispanic female in rural Colorado is brought to her primary care provider’s office with right neck pain and right-sided neck swelling of a day’s duration. The patient’s mother also stated that her daughter had a maximum temperature (T-max) of 102°F that started that morning. The patient denied any sore throat, rash, headache, rhinorrhea, cough, nasal congestion, abdominal pain, vomiting, or diarrhea. What's the diagnosis?

A healthy, afebrile, 12-month-old girl presents for evaluation with an asymptomatic nodule on her left cheek that has been present for 3 weeks. She was initially seen by her pediatrician, diagnosed with cellulitis, and prescribed an oral antibiotic, which was not administered by her parents.

A healthy 5-week-old girl presents for evaluation of rapidly growing, flat-topped red papules on the left side of her face.
A 24-year-old G2P1001 African American female at 38.2 weeks of gestation was induced for labor for a fetus with prenatally diagnosed intrauterine growth restriction (IUGR). She subsequently delivered via normal spontaneous delivery. The infant initially latched well at the breast, was normoglycemic and normothermic, but shortly after birth had had a significant episode of blood-tinged emesis (not deemed to be swallowed maternal blood) and was transferred to the transitional nursery for further evaluation.

A healthy 5-year-old boy with a 6-month history of asymptomatic 2-mm to 3-mm papules on his legs presents for evaluation of a red, slightly itchy rash that just developed on the back of his right knee. What's the diagnosis?
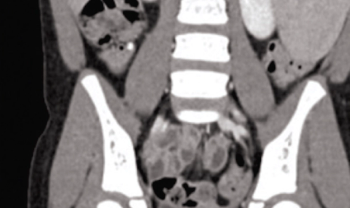
A 6-year-old female with history of previously resolved iron-deficiency anemia presents to the emergency department (ED) for numerous episodes of nonbloody, nonbilious vomiting and diffuse abdominal pain that began on the day of presentation. She had initially presented to her pediatrician who felt a large left-upper-quadrant abdominal mass and referred her to the ED for further evaluation. She has no associated diarrhea or urinary symptoms. What's the diagnosis?

An otherwise healthy 5-month-old girl presents with an asymptomatic, rapidly growing, firm, smooth nodule on the side of her left fifth finger since she was 2 months of age.