






Early exposure to peanuts has been shown to reduce the risk of peanut allergy. Is the same true with cow's milk?
Early exposure to peanuts has been shown to reduce the risk of peanut allergy. Is the same true with cow's milk?

For infants with milk allergies, finding a formula that won't cause a reaction is key to happy feeding times. Parents face a dizzying array of options. Here's a look at them.
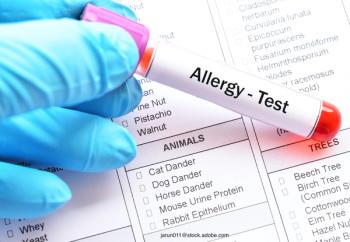
New allergy testing tools can help pinpoint exact triggers for pet allergies.

They may be our best friends and internet superstars, but pet allergies are a fact of life for many children.

When a child develops allergies to the family pet, what can the family do to help control the allergies and keep the pet in the home?

With COVID-19 still at large, pediatricians should prepare for a tough allergy season.

Climate change means more than stronger, more ferocious weather and hard-to-contain wildfires. Here's what it means for allergies.

Just because the weather cools down in the Fall months, doesn't mean that respiratory allergies are done. Here's a look at some of the best respiratory allergy remedies.

What does climate change mean for allergies and asthma in children?
Early exposure to potential allergens has been shown to help with food allergy. An investigation examines how quality of life might affect this exposure.

Though pacifiers are a comforting apparatus for many babies, they often pop out and land on the floor, requiring constant washing. A new report examines if there’s a link between pacifiers and how they’re cleaned after they hit the floor with the risk of food allergy.

A recent survey results show that cat owners who suffer from pet-related allergies are willing to do whatever it takes to keep their feline family members.

It’s springtime, which means flowers are blooming and children sneezing. Here’s a quick refresher on seasonal allergy diagnoses and prescriptions.

Emerging evidence reveals that earlier introduction of highly allergenic foods into infants’ diets may actually lead to immune tolerance. Here’s what you should know.

Spending time around animals as an infant has been suggested as a way to reduce the incidence of atopic dermatitis. An investigation offers some insight.

Guidance offers insight on allergy prevention strategies.

A new study suggests that extending early peanut introduction efforts can head off more allergy development.

Expert weighs in on adoption of early feeding guidelines for peanut allergy avoidance.

Oral immunotherapy has been an effective way to treat peanut and egg allergies. Can baked egg therapy improve food allergy outcomes in children who can tolerate baked eggs?

Peanut allergies are a big concern for parents when it comes to infant feeding. How can clinicians help?

Recent study suggests avoidance may not be the best medicine.
A study examines using oral challenges to diagnose acetaminophen ingestion allergies.
An Australian study examines how childhood wheezing can impact the development of allergies.

A research team in Australia has tied early exposure dust mite allergens through breast milk to later development of food allergies.

Contemporary Pediatrics sat down with Margaret T. Redmond, MD, a pediatric allergist at Nationwide Children’s Hospital in Columbus, Ohio, to discuss how to manage allergies in general pediatric practice and when to seek help.