
A 6-month-old boy with 1-week history of dry cough that worsened at night. He had been wheezing off and on for the past month and had visited the emergency department on one occasion.
A 6-month-old boy with 1-week history of dry cough that worsened at night. He had been wheezing off and on for the past month and had visited the emergency department on one occasion.
For decades, our country's health care system and its government have struggled with the challenge of providing immunization coverage for all children. Starting with the Section 317 legislation of 1962, numerous policy initiatives have been passed in an effort to ensure that sufficient supplies of vaccines are available, that the cost of vaccines for low–income children is covered-and that these vaccines are actually administered to the children that need them.

This baby boy was born with bilateral medial colobomas of the upper eyelids without tarsal plates and bilateral accessory tragi. Radiographs showed no vertebral anomalies, and no other physical abnormalities were evident.
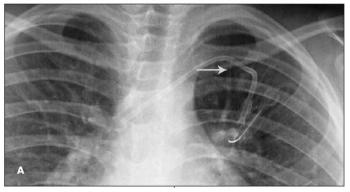
The imaging studies shown are from 2 children with cancer who underwent placement of 9.6 French left subclavian central venous catheters (CVCs) to facilitate treatment. Fracture of the catheters with subsequent embolization of the distal fragment to the pulmonary arteries was noted at about 18 months after placement. Findings suggestive of impending fracture were missed in previous radiographs. In both cases, an interventional radiologist removed the fragment via percutaneous catheterization of the right femoral vein.

Bullous impetigo caused multiple areas of denuded skin, consisting of ruptured bullae with underlying erythema, on the face, lower abdomen, and thighs in this infant.
A MOTHER ASKS: “In the past month, I’ve used a pharmacist- recommended anti-lice shampoo 4 times and my daughter still has lice. Can you call in a prescription to get rid of them?”
A 7-year-old girl presented with pain and discomfort in the left leg that was exacerbated by physical activity. She had been born with a port-wine stain on the left knee. As her mobility increased, she occasionally complained of discomfort in the left leg. Klippel-Trenaunay syndrome (KTS) was diagnosed at age 3 years after an evaluation for swelling, discoloration, and pain of the left leg. Magnetic resonance angiography and venography had revealed abnormally dilated, tortuous veins in the subcutaneous tissues from the distal thigh to the posterolateral calf with involvement of the proximal anterior tibial muscle. The parents had elected for conservative management with observation.
Two recent reports, one conducted by the Health Resource and Service Administration (HRSA)1 and a second from the CDC,2 now estimate that the current prevalence of autism spectrum disorders (ASDs) in children born in the United States has risen from 1:150 to around 1:100. The HRSA report was based on a telephone survey of 78,037 parents involved in the 2007 National Survey of Children's Health.1 However, for its study, the CDC used a rigorous identification and confirmation system called the Autism and Developmental Disabilities Monitoring Network, which cross-references educational and health data in 11 states.2
Type 1 diabetes mellitus (T1DM) is the most common type of diabetes encountered in children. The incidence of T1DM in children is increasing in some populations. Early recognition of symptoms of T1DM is critical to avoid life-threatening metabolic decompensation. Such symptoms can include polyuria, polydipsia, fatigue, weight loss, urinary tract infection, vaginal candidiasis, and “fruity” breath. In the presence of clinical symptoms of hyperglycemia, diagnosis requires just 1 laboratory blood glucose measurement above the established threshold for the child’s age. In the absence of typical symptoms, a second abnormal blood glucose measurement on a different day is needed.
Although at present there is no cure for type 1 diabetes mellitus, good treatments are available that can enable affected children to lead healthy, active lives. Insulin regimens should be designed to optimize metabolic control while minimizing the risk of adverse events, such as hypoglycemic episodes, which can be more serious in children. Regimens of 3 in- jections per day work well for children who cannot receive an injection at lunchtime, while multiple daily injection (MDI) regimens provide more flexibility. Continuous subcutaneous insulin infusion (CSII) can provide better quality of life than MDI regimens, but CSII requires a high level of motivation and carries its own risks. In all children, insulin regimens must be adjusted to accommodate the physiological changes of growth and development. Long-term follow-up is important to monitor for complications of diabetes.

An 8-year-old girl presents with a 1-year history of the progressive development of multiple 5- to 8-mm hypopigmented macules all over her body. Her parents do not recall any other skin changes, and no other skin changes are evident on presentation.
A 6-year-old boy presents with tall stature (97th percentile for age), motor delays (walking at 16 months), speech delays (expressive vocabulary of 30 to 40 words with recent use of 2-word phrases), and behavioral differences (poor eye contact, lack of pointing, hyperactive behavior with hand-flapping).
I appreciated Dr Kirk Barber's excellent illustration of a branchial cleft sinus ("Dermclinic," CONSULTANT FOR PEDIATRICIANS, November 2009, page 389).