
A healthy 3-year-old girl presents for evaluation of light brown spots on her trunk and extremities that have appeared over the last 2 years. The spots are not symptomatic but the girl’s parents are worried that she could have neurofibromatosis.
A healthy 3-year-old girl presents for evaluation of light brown spots on her trunk and extremities that have appeared over the last 2 years. The spots are not symptomatic but the girl’s parents are worried that she could have neurofibromatosis.

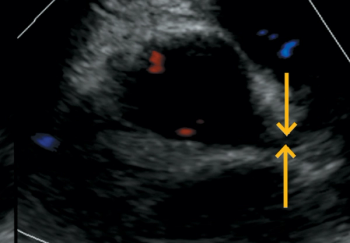
A previously healthy 15-year-old female presents to the emergency department (ED) with complaints of right-sided neck swelling, pain, decreased range of motion, and fever for 3 days. She also reports a sore throat and mouth pain with decreased oral intake. She denies any rhinorrhea, shortness of breath, difficulty swallowing, vomiting, or dental pain. What's the diagnosis?
A 3-year old male presents with 3 days of fever (maximal temperature, 105°F), diffuse abdominal pain, and several episodes of nonbilious, nonbloody emesis and loose nonbilious, nonmucousy stools. On day 3 of illness, he was seen at an urgent care clinic where he was diagnosed with acute otitis media and prescribed amoxicillin and ondansetron. He could not tolerate any oral intake and developed red eyes, abdominal pain, and redness of his hands and feet. Later that same night, he presented to the pediatric emergency department and was admitted to the pediatric ward for management of his fever, abdominal pain, and dehydration.

A 3-month-old boy presents for evaluation of a diffuse asymptomatic rash that began on his scalp and skin creases 6 weeks ago and has spread over his trunk and extremities. This week he has begun to scratch at his neck and abdomen.
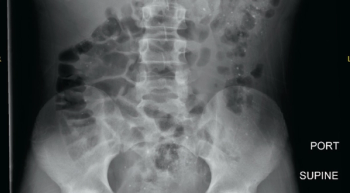
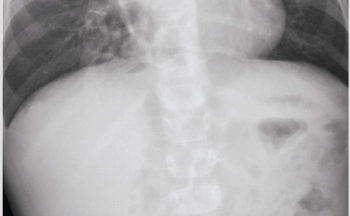
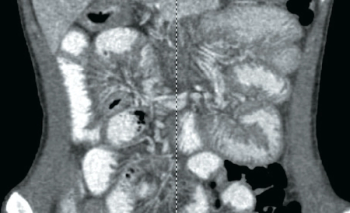
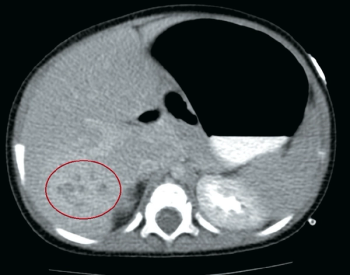
An 11-year-old male presents to the emergency department (ED) with complaint of 2 days of focal, crampy, periumbilical abdominal pain associated with anorexia, fever, and 1 episode of emesis. What's the diagnosis?

A healthy 14-year-old girl with a progressive asymptomatic rash on her arms, legs, trunk, and face presents for evaluation. She was treated for eczema with minimal improvement.

A healthy 12-year-old girl presents to the clinic with 2 days of low-grade fever and enlarging, painful, tense bullae on both hands. She had recently been diagnosed with streptococcal pharyngitis and was being treated with oral cefixime.

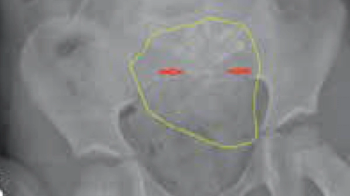
A 15-year-old adolescent Caucasian male with no significant past medical history presented to the clinic with gradually worsening left ankle pain over the past 2 weeks, ever since he started his football practice. He complained of dull aching pain at the lower end of his left leg for the past 4 months, which was slightly relieved by over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs). He twisted his left ankle and noticed further worsening pain, which prompted this doctor visit.

A healthy 11-year-old boy is brought to the office for evaluation of asymptomatic reticulated rash that started on his ankles 3 weeks ago and since has spread to his shins and the tops of both feet. He is on no medications and has had no history of trauma or recent illness. What's the diagnosis?

The patient, an 8-year-old male who recently immigrated to the United States from El Salvador, initially presented to the emergency department (ED) for a cough. The next day, he went to the general pediatrics clinic for follow-up and was noted to have a significant history of recurrent fractures.
A 4-year-old girl presents to the emergency department (ED) with a 12-hour history of progressively worsening episodic left lower quadrant (LLQ) abdominal pain and nonbilious emesis. There was no history of fever, diarrhea, hematochezia, constipation, or dysuria. The child was previously healthy, did not take any medications, and had no history of prior surgery.

The parents of a 2-month-old boy return to the office for a well-child visit. The infant has a history of hypotonia and poor head control but is growing normally. His parents noted streaky patterns of hypopigmentation over his trunk and extremities shortly after birth and felt they were likely just “birthmarks.”
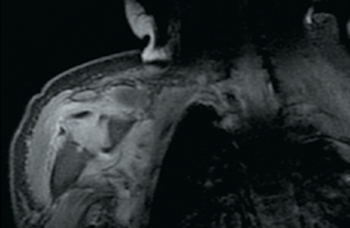
An 11-day-old, full-term male presents to the emergency department (ED) with a 2-day history of decreased range of motion of his right upper extremity.

A 16-year-old girl presents to the clinic for acne follow-up and mentions that her palms wrinkle significantly after only a few minutes of immersion in water. She is otherwise well and has no significant past medical history.
A previously healthy 4-year-old male, born late preterm by urgent cesarean delivery with an uncomplicated postnatal course, presents to the outpatient clinic for a chief complaint of worsening cough over the past 5 months. He denies current fever, rhinorrhea, shortness of breath, diarrhea, or vomiting. His cough has been worsening in severity and frequency, and mostly occurs during the daytime.

An 8-year-old boy is brought to the office for evaluation of a persistent itchy rash on his extremities, trunk, and face. Although the rash has been present for longer than 3 months, individual skin lesions change from hour to hour and occasionally the rash clears completely only to recur several hours later. He is otherwise healthy with no known allergies, changes in diet, medication use, or recent illness.

A previously healthy 8-year-old boy presents to the dermatology clinic with a progressively worsening elbow rash over the course of the last week. The rash does not itch. He spent the previous weekend sailing on the Chesapeake Bay. His pediatrician prescribed a course of cephalexin as well as a trial of topical antiviral ointment, neither of which improved the rash. The patient denies any other new exposures.
A 16-year-old male with a history of nephrotic syndrome and gastritis presents to the emergency department (ED) with worsening emesis, diarrhea, and abdominal pain of 3-weeks’ duration.

A 6-day-old, late-preterm male neonate presents to his pediatrician’s office with bilious emesis and is admitted for further evaluation. He was born at 36 weeks and 6 days via spontaneous vaginal delivery to a 23-year-old G4P4 mother with negative serologies, negative antenatal Group B Streptococcus testing, and no significant prenatal events. His stay in the newborn nursery was unremarkable. The neonate is exclusively breastfed, has no history of rectal bleeding, and passed meconium within the first 24 hours.

A 33-year-old female, G3P1011, was transferred from an outside facility at 33 weeks and 6 days gestation for anticipated preterm delivery secondary to preeclampsia. On prenatal ultrasound, her fetus was diagnosed with an omphalocele and delivery was preferred at an institution with a neonatal intensive care unit to manage the infant.
A 7-month-old girl presents to her pediatrician’s office with a 1-week history of fevers and upper respiratory symptoms. What's the diagnosis?
A 5-month-old previously healthy, full-term female presented to a pediatric emergency department with 2 weeks of left leg swelling. Her parents denied any history of trauma, pain, fevers, weight loss, and easy bruising or bleeding, and family history was negative for cancer. The patient had been feeding and eliminating well.
A 12-year-old girl is referred to the office after a routine dilated eye exam shows unusual retinal lesions. The child has been having headaches for the past 2 years that are described as mostly in the vertex with no other associated vomiting symptoms. Headaches are intermittent and usually relieved with ibuprofen.
A 5-month-old Hispanic boy, previously healthy, presents to the emergency department (ED) for 5 days of fever, 3 days of diarrhea and rash, and 2 days of vomiting. He had been diagnosed with acute otitis media by his primary care physician 3 days prior to his presentation and started on amoxicillin. The parents brought their son to the ED because of his persistent fever up to 104°F and decreased oral intake. He has no recent travel and no known sick contacts. His immunizations are up to date and he has never been hospitalized. He was born in the United States, full term with an uncomplicated birth history.
We know you love a diagnostic challenge. Can you crack these 6 puzzling cases?
An 8-year-old girl is admitted to the hospital with complaints of right ear pain, right leg pain, left arm pain, and fever after a week of worsening symptoms.
A 3-week-old female presented to the emergency department with a 3-day history of a progressively enlarging, erythematous, seemingly painful lump on her back.
A 5-month-old Hispanic male presented to the emergency department (ED) at a children’s hospital in the Northeast United States directly from his daycare after caretakers witnessed 2 shaking, seizure-like episodes. The episodes lasted 1 to 2 minutes in the setting of a fever as palpated by the parents.
A 15-year-old female presents to the emergency department of a community hospital with acute onset of duskiness in her left arm.
The father of a healthy 15-year-old girl brings her to the emergency department (ED) for evaluation of blue hands.