
Adverse events in childhood have a lifelong impact. A new study provides more evidence of negative cardiovascular outcomes.
Adverse events in childhood have a lifelong impact. A new study provides more evidence of negative cardiovascular outcomes.

Clinical trials have led to many improvements in pediatric cancer survival rates. However, a new study finds that enrollment rates in clinical trials are on the decline.

Being born very preterm (VPT) carries a number of increased risks. A new study looks at the increased risks of developing mental health disorders among children born VPR).

The new editor-in-chief of Contemporary Pediatrics shares her vision for the future.

A new report in The Lancet covers 10 pediatric cases of the pediatric multisystem inflammatory syndrome (PMIS).

Medicaid coverage provides essential care during pregnancy. Expansion of the program can impact the number of poor mothers who have no health insurance.

Encephalitis may lead to neurologic morbidity and mortality in children. Early etiologic diagnosis is important to improving outcomes.

A new report from Centers for Disease Control and Prevention’s National Center for Health Statistics examines adolescent sexual activity and contraception use.

Making the move to telehealth has many considerations. Here are 5 to keep in mind when making the transition.

Past studies have shown COVID-19 to be milder in children. However, there have been a growing number of children in New York City and Long Island in New York who have developed a multisystem inflammatory syndrome as a result of the disease.

Current US vaccine policy recommends that children receive 2 influenza vaccine doses during their first influenza season. A new study indicates that this helps reduce influenza burden among the vulnerable population.

Long recommended to improve health outcomes in infants, tummy time may have other positive health benefits, according to a new literature review.
Improving care and tackling the cost of care have been the biggest challenges in health care. A new study examines if improvement initiatives also have potential financial benefits.

Schools have closed for the academic year, but in preparation for the fall term the American Academy of Pediatrics (AAP) has offered guidance on what to consider before schools reopen.
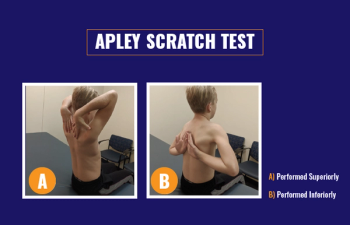
Physical exams for shoulder pain in young athletes can be performed in the primary care setting. Here are 6 tests to help diagnose the source of the pain.

The first large-scale study of pediatric sedation examines the major trends in outpatient procedural sedation.

It’s time to recognize a national treasure-nurses-during National Nurses Month. We can’t hug them during these days of social distancing, but we can honor them and thank them for all that they do, especially at great personal cost.

Suicide in children and adolescents is a serious public health problem. Researchers looked at one way to help reverse current trends.
Paternal smoking before conception or during pregnancy are both associated with increased risk of acute lymphoblastic leukemia in offspring, and the risk is significant when daily smoking consumption is higher than a certain threshold, according to a recent meta-analysis.

Children who have acute lymphoblastic leukemia (ALL) can reduce their risk of infection by consuming a diet rich in fruits and vegetable, according to a new 2-year cohort study.

Data from China had indicated a milder disease course overall in pediatric cases and now new data from Italy continues to confirm that conclusion.

A study in children with asthma showed that a medical and behavioral intervention program delivered by video-based telehealth is feasible and can significantly improve asthma outcomes and care.

The American Academy of Pediatrics (AAP) has issued a new clinical report on promoting sexual and reproductive health in adolescent males.
A retrospective study in 73 patients aged from 5 to 20 years who underwent laparoscopic appendectomy found that after hospital discharge (within 2 days of surgery) most patients had adequate analgesia without being prescribed opioids.

A new study adds to previous research on the impact of exposure in utero to antidepressants.

The front line of the COVID-19 pandemic is a dangerous place. A new study highlights just how many health care workers are at risk of poor outcomes.
As pediatric cases of COVID-19 grow, a new study warns that pediatric care centers could become overwhelmed.

The development of congenital heart disease has many potential factors. New research indicates that maternal exposure to pollutants and deprivation can increase the risk of the disease for their offspring.

Long-term counseling about diet can have a positive effect on adult cardiometabolic health, according to a new study.

Curious children are getting into their homes’ COVID-19 cleaning supplies and disinfectant products at an alarming rate, according to data from US Poison Control Centers and the Centers for Disease Control and Prevention.