



A 5-year-old boy was brought for evaluation of ongoing thrombocytopenia before undergoing adenotonsillectomy for obstructive sleep apnea. The child had been given a diagnosis of "growing pains" after frequent evaluation for leg pain over the past 2 years.
Dermatology
Latest News
Advertisement
Advertisement

A 2-year-old boy brought for pediatric dermatology consultation because of the "worst diaper rash in the world." Mother reported that the rash had been present for a year and was asymptomatic. She had been using topical barrier creams, corticosteroids, and antifungals to treat the area. Child had also received a course of oral antibiotics. Occasional improvement of rash noted but never complete resolution. Patient had no other medical problems. Family history noncontributory.

In early summer, an 8-year-old boy from rural central Virginia was brought for evaluation of a rash on his buttock. He had noticed the rash that morning, when it became pruritic. The father had removed a tick from the area about 10 days earlier. The child denied fever, headache, vomiting, fatigue, arthralgia, myalgia, and other symptoms.
The American Academy of Pediatrics (AAP) recently doubled the amount of vitamin D that it recommends all infants, children, and adolescents receive each day-from 200 to 400 IU. Also new is the academy's recommendation that vitamin D supplementation begin as soon after birth as possible. Supplementation is recommended in infants who do not receive 400 IU per day from formula.
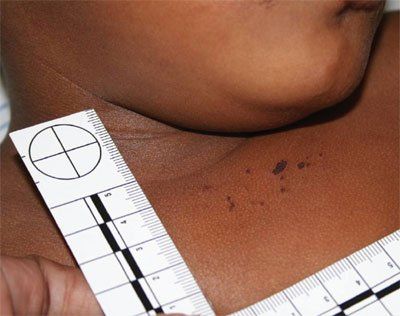
An 18-year-old girl presented for evaluation of several pink, crusted papules with surrounding hyperpigmentation and a larger pink, crusted nodule with purulent drainage on her inferior right knee

The parents of this 8-year-old boy consult you about the warts on their son’s hands. During the examination, you discover multiple sharply defined light brown flat papules on the child’s forehead.
Three profiles of a magical waste basket, a reusable breastpump, and a t-shirt that helps prevent food allergies.
Teen with painful papules and plaques is diagnosed with Sweet's Syndrome
The ninth in a year-long series of commentary reviewing topics published in Contemporary Pediatrics 25 years ago. This month's article reviews the causes and management of hirsutism in adolescent girls.
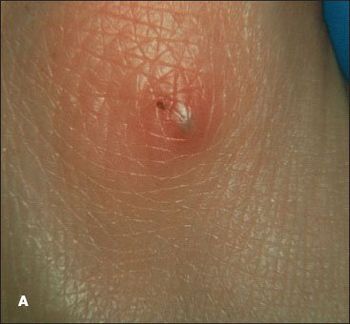
Purpuric pustules can present diagnostic challenges. However, the ability to correctly identify these lesions can be of crucial-even lifesaving-importance in caring for ill children.

Erythematous pustules and papules with some coalescence developed on the anterior trunk and to a lesser degree on the face and extremities of a newborn boy the day after birth. The baby was born at full term after an uncomplicated pregnancy and delivery.

An apparently healthy 9-year-old girl noted to have left ankle mass during well-child checkup. Her last well-child visit was 3 years earlier. Medical history unremarkable. She denied fevers, weight loss, night sweats, and chills. No family history of bone deformities or growth disturbances.
Few clinical scenarios engender as much anxiety as the sudden onset of rash and fever in a child. However, the diagnostic possibilities can be quickly narrowed-and the likelihood of potentially serious disease can be assessed-with a triage system that involves classifying the presenting symptoms into 1 of 3 groups.
A 10-week-old white baby girl with a history of difficulty in breathing presented with stridor, tachypnea, wheezing, and increased work of breathing.
A child is born with congenital melanocytic nevi.
A 3-year-old boy with white patches on the trunk first noticed shortly after birth.
A 17-year-old girl presented for evaluation of right hip pain. Several months earlier she had incurred a twisting injury to her hip when she landed from a jump while dancing.

Episodic right-sided facial flushing was noted in a 2-month-old girl born at full term via forceps-assisted vaginal delivery. The erythema appeared within minutes of latching onto her mother’s breast and resolved within 5 to 10 minutes after breastfeeding. The episodes of flushing had begun a week before the clinic visit; there were no collateral symptoms of anaphylaxis. Because food allergy was suspected, the mother had eliminated all dairy products from her diet.

A 7-year-old boy was brought for evaluation of a nonpruritic, nonpainful, evolving polymorphic rash that began on the torso and spread to the extremities, face, palms, and soles over a 2-week period. He had been otherwise healthy and had no history of constitutional symptoms.

Circumscribed erythematous lesions developed on the back and abdomen of this 19-month-old boy. The rash was mildly pruritic. The parents gave the child 1 dose of diphenhydramine, and the rash resolved after an hour. About 12 hours later, new lesions developed on the face, neck, and upper back. The child was given the same treatment and the symptoms resolved. The following morning, widespread lesions were noted on the child's face, neck, trunk, and extremities.
It was hit by two hurricanes in September 2008 -- one literal and one financial -- but the Shriners Hospital for Children in Galveston will be reopening.
A 7-month-old child appears at the derm office with a blistering eruption that started six days before on her face and neck, and has spread to trunk and extremities.

The parents of this 6-year-old girl expressed concern about a yellow-brown arciform plaque on their daughter's cheek that has been present since birth. Although it has remained stable throughout her early childhood, her parents wonder whether it may become cancerous later on. Would you recommend removing the lesion?
Although it has been more than 40 years since Kawasaki disease was first described, it is still something of a medical mystery.
In his Dermclinic case in the March 2009 issue of CONSULTANT FOR PEDIATRICIANS (page 77), Dr Kirk Barber discusses juvenile plantar dermatosis (JPD). A very simple treatment for this condition is the use of a home foot spa, in which wax is melted and the foot immersed according to the directions included with the device. Following the wax immersion procedure, the patient should apply a good lotion. JPD can be remedied or at least controlled with this treatment.
Advertisement
Advertisement
Trending on Contemporary Pediatrics
1
FDA approves acetaminophen-naproxen sodium combination tablet for ages 12 and older
2
US measles cases surpass 2025 total, hit highest level since 1991
3
Pooled phase 3 data show early, consistent tapinarof cream responses across pediatric age groups in AD
4
Individualized gene therapy shows early promise for SCN2A-related epileptic encephalopathy
5